Is it Time for a Medical Readiness Availability Rating?
Franklin C. Annis
There is a continual push to ensure maximum Medical Readiness within the U.S. Army. But there is a question if the current methods of assessing readiness is providing the information required to determine efficiency. A recent article describing the possibility of adding an availability assessment (A-Rating) in Marine Corps Logistics might provide an inspirational source for innovation to Army medicine. Instead of capturing Medical Readiness as individual “snap-shots” in time, it might be more accurate to measure Medical Readiness over time. If the mission of the Army Medical Department (AMEDD) is to “conserve the fighting strength,” I could think of no better measurement than the concept of availability. If sustained Medical Readiness is the ultimate goal, the Army should have an assessment measure to match this objective.
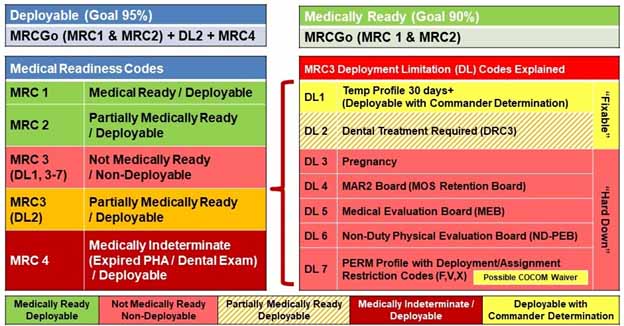
Figure 1 - Medical Readiness Smart Card
As explained by Fincher, availability rating is calculated through the following formula: “A-Rating = (Total Time – Downtime) / Total Time.” (2019, para. 4). A perfect score would yield a result of “1”. The more days of downtime in this equation the closer the score would approach zero. In the Medical Readiness context, an Availability Rating could be established by the days in the Medical Readiness Code 1 or 2 (a.k.a. “MRC Go”) divided by the total time. If we included days of profile in this calculation, there are further benefits explained below. The reason why we might consider adding an A-Rating to how we measure Medical Readiness is that it could provide a great number of insights into the causes of decreased Medical Readiness. An A-Rating could reveal the inefficiencies within our Medical Readiness support operations, provide some concept of the command emphasis placed on Medical Readiness, the degree of individual Soldier compliance, and better understanding of the cost of Medical Readiness. With these types of insights, we would be in a position to better support Medical Readiness operations, explain the factors currently influencing our current status, and better estimate additional resources required to meet specific goals.
We will make an assumption that Army could “break” Soldiers in training. With ever increasing demands to maintain units at the highest levels of readiness, the U.S. Army is actively engaging in training. Preparing Soldiers for the modern battlefield increasingly requires realistic training scenarios that place Soldiers at a higher risk of Line of Duty (LOD) injuries. As units prepare for deployment, it would be expected that LOD injuries occur and as a result the Medical Readiness within a unit may drop. However, we would not want to “punish” commanders for accepting reasonable risk in training their Soldiers so we should account for these injuries within our availability ratings. Therefore, I would propose that we use the data of the days on profile within the Medical Operational Data System (MODS) Command Portal to determine the “gap” that might exist when Soldiers are not Medically Ready or being actively managed under a profile (MRC 3).
Examples (Measured over a Two-Year Period)
An optimal example might be a Soldier that has been MRC Go for 670 days over the last two years with the other 60 days on profile. 700 days MRC Go / 730 days = .92 Availability. 60 days / 730 days = .08 Profile (we could possibly call this a “Profile-Rating”). Since this Soldiers A-Rating + Profile-Rating equals 1, it indicates that there was no gap in medical oversight for this individual.
A suboptimal example might be a Soldier that has been MRC 4 (Medically Indeterminate) for 15 months with one 30 day profile that expired with no follow-up. (210 days MRC Go / 730 days = .29 Availability. 30 days / 730 days = .04 Profile. In this situation, the Availability + Profile rating equals .33. This would imply that there was a lack of medical oversight for this Soldier for 67% of this two year period.
It is Soldiers that present gaps in medical oversight that truly present a risk for the U.S. Army’s readiness. Gaps display periods where Soldier readiness is unknown and if injuries/illnesses exist they were not being medically managed. Even if the aggregate Medical Readiness percentage was not improved by closing this availability gap, it would be worth the Army’s investment to decrease the risk of unknown health statuses, ensure appropriate medical case management of illnesses or injuries, and identify individuals that should be removed due to the inability to maintain minimum medical retention requirements.
Runs Parallel with Current Policies and Data Collection
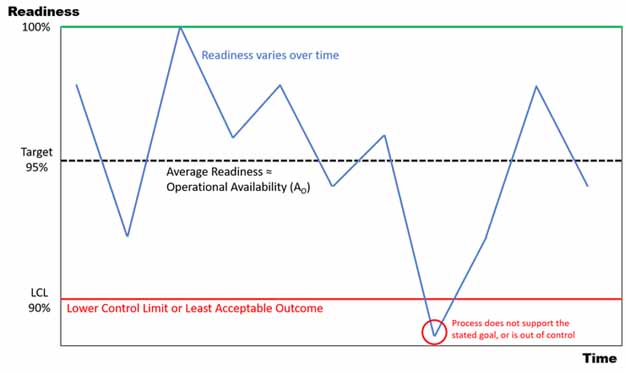
Figure 2 – Availability (Readiness / Time) (Fincher, 2019)
It is important to note that adding an A-Rating likely falls in line with current policies. The Army already has an established Medical Readiness “Target” (currently 90% MRC Go). AMEDD has an established standard for the maximum number of days on profile within the last two-years as a trigger point for a Medical Readiness Determination (MRD) to possibly start a medical board process. It could be asserted that this standard is our Lower Control Limit (LCL) in the availability paradigm. Given the Army is already capturing much of the data required to generate an A-Rating, it would take very little modification and cost to adapt the existing electronic medical tracking systems to provide this calculation.
Reasons for the Gap
Once the availability gap is determined, it will increase the ability to address some possible underlying causes. The three primary causes are likely the availability of Medical Readiness Events, commanders’ emphasis on Medical Readiness, and Soldier compliance. Having a better understanding of this gap may help to provide resources to improve availability or at a minimum provide a better understanding of why this gap is occurring.
Medical Readiness Events. One cause for this gap might be the simple lack of Medical Readiness Events for Soldiers. In the Army National Guard, if a Soldier misses a Medical Readiness Event, it is likely they will have to wait a month or more to be rescheduled. If it was determined how much of a gap this type of situation created, it could be determined if the cost of providing additional Medical Readiness Events are cost effective. In the National Guard, this information could also be used to justify fulltime employment of providers capable of providing Psychical Health Assessment (PHA) operations on a daily basis if required. This information would be invaluable to “right size” medical operations and medical units to meet the needs of the Army.
Command Emphasis. If it was determined that sufficient opportunities existed for Soldiers to attend PHAs, the emphasis on Medical Readiness could be determined. In many cases, Soldiers might be unable to attend Medical Readiness Events due to the requirement to attend training. Being able to assess the size of the gap caused by command emphasis on the importance of Medical Readiness would allow strategic leaders to assess and take action they deem appropriate. This may or may not result in more emphasis on Medical Readiness but may help to alleviate the stress of our medical personnel that are constantly providing opportunities to improve Medical Readiness but struggle to get Soldiers “through the door.”
Soldier Compliance. The availability gap created by Soldiers being scheduled for but not attending Medical Readiness Events could be determined. This gap would be useful in assessing the significance of this problem to strategic leaders to ensure commanders are provided and utilize appropriate tools to correct indiscipline within their organizations. I can see this being particularly useful to address grossly non-compliant individuals that have gone for months or years without a PHA. They would be quickly pressured to attend a Medical Readiness Event in hopes of increasing the average availability rating of an organization.
Cost
One of the greatest benefits I could see in adapting an A-Rating would be an increased understanding of the cost of Medical Readiness. With recent events such as the National Guard’s “Race to Medical Readiness”, senior leaders might ask what they “bought” with increased levels of funding. Instead of just being able to provide them with a “snapshot” Medical Readiness percentage increase valid for the day that it was pulled from MEDPROS (i.e. a 3% increase in Medical Readiness), we could communicate the impact in terms of availability. Imagine being able to say we increase the Medical Readiness of Soldiers by “x” number of days or closed the gaps in medical oversight to “x” degree? After an A-Rating system was in place for a few years, it might be a valuable tool for estimating the cost of Medical Readiness and any proposed increases. It might also be useful in displaying the impacts of the law of diminishing returns as we approach the upper limits of Medical Readiness.
AMEDD Mission
I could imagine no better way of supporting AMEDD’s core mission than by measuring medical readiness over time. It will help to further shift the paradigm from thinking about Medical Readiness as a “one-day” event to a year-round process. Imagine being about to compare units in terms of availability. Currently, we might take a look at two similar units (like Infantry Companies for example) and find they have similar Medical Readiness percentages (say 89% MRC Go). We might conclude they are similarly prepared for war. But if one had an average A-Rating of .78 while the other had an average A-Rating of .35, we might take notice that the priority and support for Medical Readiness is not the same in these two units. This might be an issue of a lack of command emphasis in one unit, an indicator of a need for more PHA opportunities/medical care in certain areas, or a signal for more preventative medicine to be employed in low A-Rating units.
A-Ratings might also be a solution to refocus commanders on their Medical Readiness with the recent policy shift towards Deployability. It might be time to think about simplifying the Medical Readiness objectives to 95% Deployability with “x” level of Availability. This could achieve the intended goals of maintaining high levels of Medical Readiness without the need for multiple different standards (i.e. 95% Deployable, 90% MRC Go, >8% MRC 3, >2% MRC 4). Simplifying Medical Readiness to just two requirements (Deployability and Availability), might go a long way to “demystifying” our Medical Readiness requirements in the Army as a whole. It would drive home the point that Soldiers need to be Medically Ready and stay Medically Ready.
Conclusion
If the Army seeks to provide a Medical Ready force now and in the future, we must account for time. Adding an availability assessment to Medical Readiness will allow us to better determine gaps in medical oversight and seek creative solutions. An availability assessment would greatly aid in determining the impact of initiatives and aid in accurate determination of the cost/benefit of our actions. The cost of adding such an assessment would be minimum with the vast amount of data and policies need to support such a measurement are already in existence. The benefit of this assessment method would be great as it would continue to shift the paradigm of Medical Readiness towards a daily process. If the goal of AMEDD is to truly “conserve the fighting strength,” it is time we utilize an A-Rating to validate how well we accomplish this task.
I would like to thank Jason Fincher for explaining the concept of availability to me at an Association of Marine Corps Logisticians event. Jason is one of the founding members of this organization and it is specifically these types of private organizations that provide “safe spaces” to explore creative and innovative ideas. I look forward to seeing the great ideas that are bound to come out of this group of dedicated professionals.
References
Coleman, Amber. “The A-Rating”, Marine Corps Gazette, March 2019, https://mca-marines.org/gazette/the-A-Rating/
Fincher, Jason. “How to Fight the A-Hole in Equipment Readiness”, Association of Marine Corps Logisiticans, 2019, https://www.marinecorpslogistics.org/blog/how-to-fight-the-a-hole-in-equipment-readiness
About the Author(s)
Comments
There's always time for that…
There's always time for that. With so many problems in the world, I think medicine has to work to its fullest potential. So, for example, I'm studying to be a nurse, and I know that a lot will depend on me. So I'm totally committed to my studies. I often write papers on nursing because it's an important part of my job. In any case, I think that I will become a great professional who will help a lot of people