Casualty Aversion, The Challenge in Medical Planning for LSCO
Jennifer Wilson
Introduction
General Robert E. Lee once said, “To be a good soldier, you must love the army. To be a good commander, you must be willing to order the death of the thing you love”[i]. As simply stated, as this contradiction of sentiments, the characteristic of casualty aversion is woven into the American way of war. As such, the United States military finds itself preparing for large-scale combat operations (LSCO) with peer threats without the ability to mitigate loss of life in the vast numbers predicted, and the unwillingness to accept it. In counterinsurgency, medical planners intended to alleviate all combat losses, where a LSCO war challenges medical planners to stand in the gap between our way of war and the realities of LSCO. Future military success hinges on the American military’s ability to understand the underpinnings of casualty aversion as a component of the American way of war and be able to accept more risk with health care assets on the battlefield. This essay describes the American way of war, the development of casualty aversion, and its implications for LSCO.
The American Way of War
The American way of war, or culture of war as explained by Adrian Lewis, describes the way that Americans approach how the American military is resourced and utilized in modern warfare.[ii] To apply Edgar Schein’s culture model, the American way of war governs the basic underlying assumptions about how America conducts warfare.[iii] These basic underlying assumptions have become ingrained in the way diplomats, generals, and the people view military force. It emerged out of the Western way of war characterized by technology, discipline, highly aggressive military tradition, emphasis on innovation, and a unique system of war finance.[iv] But by America’s entrance into World War II (WWII) in 1941, the American way of war shifted to include a unique political environment, belief in technological dominance, and casualty aversion.[v] Following the military drawdown after the end of the U.S. involvement in Vietnam in 1973 the way of war changed to include a focus on small size, all-volunteer, and a cultural separation from the populace.[vi] All of these things effect the way America views casualties in combat.
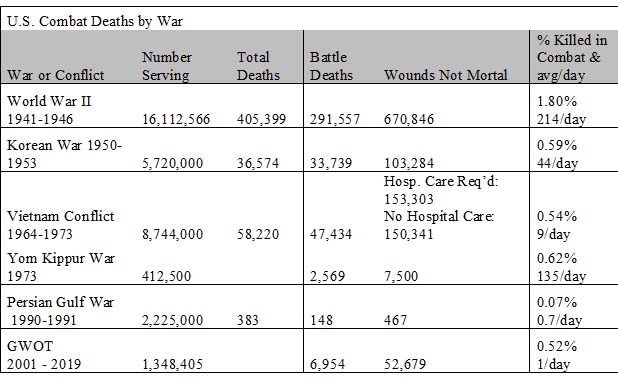
Military conflict since 1941 refined America’s casualty aversion from the desire to save America’s sons in WWII to a necessity framed by a small force and limited warfare in Korea and Vietnam. The military drew down from over three million personnel to only two million by 1975 then less than 1.5 million in 1998.[vii] The shifting way of war including limited warfare and the smaller force underscored the increased emphasis on preserving life in combat. During this time period there was a clear shift to increased focus on casualty treatment and evacuation to include the golden hour evacuation standard.[viii] The focus was further intensified in the Persian Gulf War and the Global War on Terror, where short duration battles reigned, and survival rates soared.
The Emergence of Casualty Aversion in The American Way of War
In WWII 19% of injured service members died on the battlefield or of wounds in a hospital.[ix] Units in battle focused on casualty evacuation rather than treatment, but still validated rudimentary medical-evacuation or MEDEVAC. D-Day’s Omaha Beach landing for example, used landing craft to provide en route care back to the ship and in Burma the military executed the first helicopter evacuations of wounded from hillsides.[x] Though the military did not prioritize combat medicine, the American populace still supported the war and was prepared to serve as replacements which further enabled the expenditure of casualties.
- DeBruyne, Nese F., “American War and Military Operations Casualties: Lists and Statistics,” Congressional Research Service, September 14, 2018, www.crs.gov. RL32492.
- Smith, Stew, "The Cost of War Since September 11, 2001," The Balance Careers, November 1, 2018, https://www.thebalancecareers.com/the-cost-of-war-3356924. Accessed 22 MAY 19.
During the Korean War, Task Force Smith lost 28% of its fighting force when thrust against the Democratic Peoples’ Republic of Korea (DPRK) forces that advanced through Osan over two days. The dismounted force was only minorly successful at delaying the attack of tank columns for about six hours without any medical or resupply plan.[xi] As the Korean War progressed, U.S. forces faced diverse climates, terrain, and a range of adversary capabilities which exacerbated injuries and deaths. This environment enabled medical personnel to prove the concept of helicopter evacuation and the Mobile Army Surgical Hospital (MASH), dynamically decreasing died of wounds rates from 4.5% in WWII to 2.5%. Over the course of the three-year war the U.S. suffered only 36,574 combat deaths.[xii] The low number of Americans lost reflects a shift to limited warfare with a smaller fighting force for which fewer Americans supported. The smaller committed force additionally increased awareness to preserve itself through medical treatment and evacuation processes.
Similarly, the battle at Hue in Vietnam, fought as a part of the Tet offensive lasted just over a month and cost the U.S. about 600 dead and 3,000 wounded. This casualty rate was three times the average rate throughout the entire conflict.[xiii] Hue made casualty evacuation difficult as the People’s Army of Vietnam infiltrated the complex system of walls in the Citadel extending the time from point of injury to medical attention. This tested the Marines’ ability to perform care under fire and buddy carries within the city while the war overall dramatically refined the role of “air MEDEVAC”. As a result of the Vietnam War, the expectation for evacuation from the point of injury was born because the U.S. experienced general air superiority. And as war grew more and more limited, the requirement for medical support grew more robust.
The Persian Gulf War and the Global War on Terror (including both Iraq and Afghanistan) enjoyed continued increased survival rates as well, reaching a 98% survival rate if a casualty could reach a Role III treatment facility (a field hospital with definitive surgical care) in 2015. The Persian Gulf War casualty planning estimates resulted in an overcompensation of deployed medical assets. Because the military experienced rapid and overwhelming mission success the brief war produced less than 1% U.S. combat casualties. All the while, the deployed force experienced numerous issues regarding evacuation and transportation. Had the armed conflict persisted to it predicted duration and intensity, medical and logistic capabilities may have been strained. Forces were unable to drive ambulances across the terrain and unable to employ air MEDEVAC due to visibility issues. Additionally, hospitals were unable to keep up with the maneuver forces and were more than 100 miles away from the first considerable contact.[xiv] However the military success and low number of combat casualties supported the notion in the way of war that limited warfare ought not produce high casualty numbers. This war followed by the Global War on Terror solidified the ideal that lives do not have to be lost in American warfare. As stated by the Army Surgeon General, “A Soldier with a head wound in Afghanistan could arrive from the point of injury to Bethesda Naval Medical Center where the medical specialist was standing by within 24 hours of being wounded.”[xv] Our ability to evacuate and stabilize combat casualties in the Global War on Terror has produced an unrealistic expectation of life preservation in future LSCO.
Casualty Aversion and Large-Scale Combat Operations
Furthermore, current research indicates that to have the best chance at mitigating loss of life, injuries require intervention (that is some sort of medical assessment and accurate treatment for the injury type such as a tourniquet or needle chest decompression). within the first 10 minutes.[xvi] These types of interventions are not likely in a LSCO environment. The 1973 Yom Kippur War provides a glimpse of what punctuated LSCO can produce for casualties. This and analysis of a Command and General Staff Officer College (CGSOC) warfighter exercise provide medical professionals an idea of the types and numbers of casualties need to be planned for in future combat.
An example of peer to peer LSCO, the 1973 Yom Kippur War demonstrated how complete domination can occur precisely and quickly. In this war, Israel suffered 2,569 killed and 7,500 wounded in the three-week conflict. Syria lost an estimated 3,500 dead, with 21,000 wounded. Egypt had an estimated 15,000 killed and 30,000 wounded.[xvii] This war drove home the concept of combined arms and demonstrated the lethality of air power, air defense, tanks and infantry together as well as the element of surprise.[xviii] As a result, neither side had a defined medical evacuation plan at the time of attack and has since led to the Israelis redefining military medicine.[xix] Israel’s casualties are equivalent to losing half of a Brigade Combat Team (BCT) in only three weeks, while Egypt suffered numbers equivalent to losing a division.
CGSC Estimated Warfighter Casualties and Observations
Even more eye-opening, during a brief LSCO warfighter exercise conducted during CGSOC, there were far fewer killed and died of wounds during the 18-hour battle than estimated, but the simulation produced overwhelming numbers wounded at every echelon of care. A division without any additional medical assets can effectively hold up to 60 casualties for 72 hours. There is also no surgical capability. However, in this scenario, and as might be expected in a LSCO-type deployment, the division had six Forward Resuscitative Surgical Teams (FRST) providing two surgical beds, each forward deployed the maneuver BCTs. In addition, there was one designated Field Hospital with 240 beds and two operating tables in the Corps Support Area. Lastly, the Division was augmented with two additional Role II capabilities in the division support area, which lacks surgery, but provides an additional 40 beds for patient hold. For this scenario we had 14 surgical beds and 340 bed spaces. The sheer volume logistically and a surgeon’s ability to perform multiple back to back surgeries would prove problematic. But to include the non-surgical units ability to properly triage and ground evacuate, as well as move a casualty far enough back on the battle field to be evacuated to a fixed facility by fixed wing aircraft creates a problem set that is irreplicable in training and personnel intensive in battle.
Though the simulation did not replicate casualty evacuation from the point of injury to the appropriate level of care, assets required to move over 1,100 casualties without (or even with) air MEDEVAC far exceed that which existed even with the medical augmentation in this scenario. On top of which most deaths occur due to a lack of medical intervention within the first 10 minutes of wounding, while the next biggest differential occurs around the 90-minute mark. These rates put tremendous stress on units in contact to perform sophisticated medical care and evacuation. Historical planning estimates say 15% of the fighting force will be killed in action, 85% will be wounded in action and 80% of those evacuated beyond the division organic care would require surgery. In this scenario, that would mean there would have been 935 wounded and 636 surgical cases in just 18 hours. With non-stop surgery, the 14 operating tables would have operated on 126 patients in 18 hours, leaving the remaining 610 awaiting definitive care.[xx] Rather than postulate that we ought to put more medical capability on the battlefield, military leaders, politicians, and the populace have to understand that when the U.S. goes to war with Russia, China, or another near peer, American lives will be lost. Lots of American lives will be lost as happened in WWII or in the Yom Kippur War. Medical planners have to be able to articulate these estimates and position medical assets in the best places on the battlefield as possible; but senior leaders cannot be afraid of losing ground evacuation assets, air MEDEVAC aircraft, or medics either. Military leaders should not be afraid to put medical assets closer to the fight if it means saving more lives.
Conclusions
Casualty aversion transcends the rest of the characteristics of the American way of war. In Schein’s analysis of culture, this aspect of the American way of war fits all three levels: artifacts, espoused beliefs and values, and basic underlying assumptions.[xxi] Casualty Aversion is derived from three places: the idea that the American people will not accept the losses, the ingrained military value to “not leave a fallen comrade,” and the reality that with an all-volunteer force, the U.S. cannot raise enough people to fight in a LSCO if predicted numbers of casualties prove true. Though the military’s mantra to “not leave a fallen comrade” is fueled by emotional connectedness, there is also the reality that the all-volunteer force is expensive and limited. This aspect entangles itself with the dynamic political environment of the American way of war.
After the transition to limited warfare and further solidified with the transition to an all-volunteer force, the American populace became disconnected from those in service. Ultimately, most Americans will only truly care that lives are lost when they are asked to become the replacements. While high casualty numbers are not a guarantee in LSCO, it certainly contributes to the military’s desire to win quickly, decisively, and without expending many lives.
In summary, the American way of war is mismatched against our future LSCO predicament. Perhaps if we truly love our people, we should be more willing to order the thing that which we love to its death. This conundrum of balancing our medical capability with LSCO and the American way of war is the struggle of the future medical planner in the U.S. Army. Tactics, weaponry, and terrain of the future combat environment remain unconfirmed as well as or whether there will continue to be small limited wars or peer to peer LSCO. What is apparent, however, is that the next fight will not be that of the past. If the U.S. engages in peer to peer conflict, there will likely be large amounts of casualties very quickly. Regardless of how good the evacuation plans are, the sheer volume will overwhelm even the best medical facilities. As the U.S. military continues to train for a LSCO fight, medical planners and leaders need to prepare to lose Soldiers, because casualty aversion will not save lives.
End Notes
[i] Robert E. Lee, Notable Quotes from Robert E. Lee. https://www.historynet.com/robert-e-lee-quotes. Accessed: 30 JAN 19.
II Adrian R. Lewis, The American Culture of War: The History of U.S. Military Force from World War II to Operation Enduring Freedom. (New York, NY: Routledge, 2018). 13-22.
III Edgar H. Schein, "The Role of the Founder in the Creation of Organizational Culture." MIT: School of Management. March, 1983.
IV Geoffrey Parker, The Cambridge History of Warfare, New York, NY: Cambridge University Press, 2005. 1-11.
[v] Antulio J. Echevarria II, Toward an American Way of War. Strategic Studies Institute, US War College, Carlisle, PA, March 2004.
Antulio J. Echevarria II, “What is Wrong with the American Way of War?” Prism, 3, No.4, National Defense University, April 2014: 109-115.
[vi] Lewis, The American Culture of War. 13-22.
David Coleman, “US Military Personnel 1954 – 2014,” https://historyinpieces.com/research/us-military-personnel-1954-2014. Accessed: 19 APR 19.
[vii] David Coleman, “US Military Personnel 1954 – 2014,” https://historyinpieces.com/research/us-military-personnel-1954-2014. Accessed: 19 APR 19.
[viii] Jonathan E. Clarke, LCDR, MC USN; Davis, Peter R., Lt Col, RAMC, “Medical Evacuation and Triage of Combat Casualties in Helmand Province, Afghanistan: October 2010 – April 2011,” MILITARY MEDICINE, 177, 11:1261-1262, 2012
V David Brown, “In Afghan war, rate of post-injury survival rises” January 30, 2012. https://www.washingtonpost.com/blogs/checkpoint-washington/post/tending-to-war-casualties-and-getting-better-at-it/2012/01/29/gIQAQX9saQ_blog.html?noredirect=on&utm_term=.23a1089fd26a. Accessed: 26 MAR 19.
VI David M. Lam M.D., M.P.H., Colonel, Medical Corps U.S. Army, “Medical Evacuation, History and Development-The Future in the Multinational Environment,” From: The Impact of NATO/Multinational Military Missions on Health Care Management. September 6, 2000. Medical Staff Officer, International Military Staff Headquarters NATO: Brussels Belgium: 19-5.
VII Herbert Kikoy, “Task Force Smith – America’s Entry into Korean War,” June 19 2018. https://www.warhistoryonline.com/instant-articles/task-force-smith-americas-entry.html. Accessed 19 MAR 19; Roy E. Appleman. “American Ground Forces Enter the Battle.” South to the Naktong, North to the Yalu, June to November 1950. Washington, DC: Center of Military History, United States Army, 1992: 59-76. Accessed 15 DEC 18. https://history.army.mil/books/korea/20-2-1/SN06.HTM.
VIII Nese F DeBruyne, “American War and Military Operations Casualties: Lists and Statistics,” Congressional Research Service, September 14, 2018, www.crs.gov
RL32492; Millet, Allan R. “Korean War: 1950 – 1953,” May 14, 2019. https://www.britannica.com/event/Korean-War. Accessed: 19 MAR 19; Dwight J. Zimmerman, “Battlefield Medicine in the Korean War,” February 9, 2014. https://www.defensemedianetwork.com/stories/battlefield-medicine-in-the-korean-war/. Accessed: 24 MAR 19.
IX “Battle of. Hue: American Casualties,” Honorstates.org. https://www.honorstates.org/index.php?page=features&tid=1426. Accessed: 19 MAR 19; Nese F. DeBruyne. “American War and Military Operations Casualties: Lists and Statistics,” Congressional Research Service, September 14, 2018, www.crs.gov
RL32492: 42.
XI United States General Accounting Office, “Operation Desert Storm: Full Army Medical Capability Not Achieved,” Report to the Chairman, Subcommittee on Military Personnel and Compensation, Committee on Armed Services, House of Representatives. August, 1992.
[xv] LTG Nadja Y. West, “Survival rates improving for Soldiers wounded in combat, says Army surgeon general,” by David Vergun, 24 August, 2016. https://www.army.mil/article/173808/survival_rates_improving_for_soldiers_wounded_in_combat_says_army_surgeon_general. Accessed: 16 MAY 19.
[xvi] Frederick B. Rogers, MD, MS, FACS and Katelyn Rittenhouse, BS, “The Golden Hour in Trauma: Dogma or Medical Folklore?” The Journal of Lancaster General Hospital. VOL 9 – No. 1. 12, 2014.
[xvii] Associate Press, “Casualties of Mideast Wars,” Los Angeles Times. March 8, 1991, https://www.latimes.com/archives/la-xpm-1991-03-08-mn-2592-story.html. Accessed: 19 MAR 19.
[xviii] William DePuy, Implications of the Middle East War on U.S. Tactics, Doctrine and Strategy, Command History Office, TRADOC, Fort Monroe, VA (1974). 76-85.
[xix] Ronald Chang, MD, Brian J. Eastridge, MD, John B. Holcomb, MD, “Remote Damage Control Resuscitation in Austere Environments,” In Wilderness and Environmental Medicine, 28, S124-S134 (2017).
[xix] Edgar H. Schein, L105 Reading A: “Organizational Culture and Leadership”. 4th edition. Chapter 1, “The Concept of Organizational Culture: Why Bother?”. Chapter 2, The Three Levels of Culture. CGSOC:11.
[xx] Percentages are from MCOAT Multi-unit estimator version 4.
Bibliography
Electronic and Web-based Sources
Associate Press, “Casualties of Mideast Wars,” Los Angeles Times. March 8, 1991, https://www.latimes.com/archives/la-xpm-1991-03-08-mn-2592-story.html. Accessed: 19 MAR 19.
“Battle of Hue: American Casualties,” Honorstates.org. https://www.honorstates.org/index.php?page=features&tid=1426. Accessed: 19 MAR 19.
Brown, David, “In Afghan war, rate of post-injury survival rises” January 30, 2012. https://www.washingtonpost.com/blogs/checkpoint-washington/post/tending-to-war-casualties-and-getting-better-at-it/2012/01/29/gIQAQX9saQ_blog.html?noredirect=on&utm_term=.23a1089fd26a. Accessed: 26 MAR 19.
Coleman, David, “US Military Personnel 1954 – 2014,” https://historyinpieces.com/research/us-military-personnel-1954-2014. Accessed: 19 APR 19.
Kikoy, Herbert, “Task Force Smith – America’s Entry into Korean War,” June 19 2018. https://www.warhistoryonline.com/instant-articles/task-force-smith-americas-entry.html. Accessed 19 MAR 19.
Lee, Robert, Notable Quotes from Robert E. Lee. https://www.historynet.com/robert-e-lee-quotes. Accessed: 30 JAN 19.
Millet, Allan R. “Korean War: 1950 – 1953,” May 14, 2019. https://www.britannica.com/event/Korean-War. Accessed: 19 MAR 19.
Smith, Stew, "The Cost of War Since September 11, 2001," The Balance Careers, November 1, 2018, https://www.thebalancecareers.com/the-cost-of-war-3356924. Accessed: 02 MAY 19.
Zimmerman, Dwight J. “Battlefield Medicine in the Korean War,” February 9, 2014. https://www.defensemedianetwork.com/stories/battlefield-medicine-in-the-korean-war/. Accessed: 24 MAR 19.
Books
Adrian R. Lewis, “The American Culture of War: The History of U.S. Military Force from World War II to Operation Enduring Freedom.” (New York, NY: Routledge, 2018). 13-22.
Parker, Geoffrey. The Cambridge History of Warfare, New York, NY: Cambridge University Press, 2005.
Articles
Appleman, Roy E. “American Ground Forces Enter the Battle.” South to the Naktong, North to the Yalu, June to November 1950. Washington, DC: Center of Military History, United States Army, 1992: 59-76. Accessed 15 DEC 18. https://history.army.mil/books/korea/20-2-1/SN06.HTM.
Chang, Ronald, MD, Eastridge, Brian J., MD; Holcomb, John B., MD, “Remote Damage Control Resuscitation in Austere Environments,” Wilderness and Environmental Medicine, 28, S124-S134 (2017).
Clarke, Jonathan E., LCDR, MC USN; Davis, Peter R., Lt Col, RAMC, “Medical Evacuation and Triage of Combat Casualties in Helmand Province, Afghanistan: October 2010 – April 2011,” MILITARY MEDICINE, 177, 11:1261-2, 2012.
DePuy, William. “Implications of the Middle East War on U.S. Tactics, Doctrine and Strategy”, Command History Office, 76-85. TRADOC, Fort Monroe, VA (1974).
Lam, David M., M.D., M.P.H., Colonel, Medical Corps U.S. Army, “Medical Evacuation, History and Development-The Future in the Multinational Environment,” From: The Impact of NATO/Multinational Military Missions on Health Care Management. September 6, 2000. Medical Staff Officer, International Military Staff, 19-5.
Headquarters NATO: Brussels Belgium.
DeBruyne, Nese F. “American War and Military Operations Casualties: Lists and Statistics,” Congressional Research Service, September 14, 2018, www.crs.gov
RL32492.
Echevarria II, Antulio J. Toward an American Way of War. Strategic Studies Institute, US War College, Carlisle, PA, March 2004.
Echevarria II, Antulio J. “What is Wrong with the American Way of War?” Prism, 3, No.4, National Defense University, April 2014: 109-115.
Rogers, Frederick B. MD, MS, FACS and Rittenhouse, Katelyn BS, “The Golden Hour in Trauma: Dogma or Medical Folklore?” The Journal of Lancaster General Hospital. VOL 9 – No. 1. 12, 2014.
Schein, Edgar H. "The Role of the Founder in the Creation of Organizational Culture." MIT: School of Management. March, 1983.
LTG Nadja Y. West, “Survival rates improving for Soldiers wounded in combat, says Army surgeon general,” by David Vergun, 24 August, 2016. https://www.army.mil/article/173808/survival_rates_improving_for_soldiers_wounded_in_combat_says_army_surgeon_general. Accessed: 16 MAY 19.
United States General Accounting Office, “Operation Desert Storm: Full Army Medical Capability Not Achieved,” Report to the Chairman, Subcommittee on Military Personnel and Compensation, Committee on Armed Services, House of Representatives. August, 1992.
Other
MCOAT casualty estimator version 4.